6 June 1944 - 25 July 1944
MEDICAL BUILD-UP
In the assault stage of the operation Field Ambulances landed with brigades and battalions as planned, and each beach group landed on D-day with a self-contained medical organisation comprising two Field Dressing Stations, two Field Surgical Units and a Field Transfusion Unit supplemented by small surgical teams.
With the exception of the right flank where the landings met opposition at LE HAMEL, field dressing stations were working and surgeons were performing operations in all the beach groups by H+90.
By D+2 it was possible to concentrate the Casualty Clearing Stations and the hospitals which began to arrive at the beach-head into three principal medical areas, HERMANVILLE, REVIERS and RYES.
By D+6 it was necessary to close down the area at HERMANVILLE to make way for the expansion of a neighbouring ammunition depot, and a new medical site was chosen at LA DELIVRANDE.
In the latter part of June a fourth area was developed near BAYEUX. The field dressing stations within the corps were situated near the casualty clearing stations and attended to the lightly wounded, exhaustion cases and sick, leaving the CCS clear to handle major casualties.
The hospitals in the rear medical areas received casualties from the corps CCS.
Early in July BAYEUX developed into the main L of C hospital area, and when HQ L of C took over administrative command of the bridgehead on 13 July it also took over the REVIERS concentration of hospitals.
The RYES area was closed down, and when, in the meantime, First Canadian Army assumed responsibility for the LA DELIVRANDE group, there remained two main hospital areas.
For most of July the Second Army hospitals remained static and in the latter part of the month closed in readiness to move forward.
EVACUATION BY SEA AND AIR
Casualty Evacuation Posts were established on each of the three beach sectors on D-day but enemy shelling caused the CEP (Casualty Evacuation Point) on SWORD sector to close down after the first few days, and all its casualties for evacuation were sent to the CEP on MIKE beach. Later the evacuation of casualties was further simplified by concentrating the casualties in JIG and MIKE beaches. This central CEP at COURSEULLES was enlarged and formed out of two FDS, two FSU and one FTU. It had accommodation for 1,500 casualties and held cases until shipping and weather permitted evacuation.
Evacuation to UK was carried out by means of LSTs modified to carry stretcher cases, hospital carriers and medically manned LSTs for walking wounded. These were loaded initially off-shore by DUKWS specially allotted for medical purposes.
On D-day and D+1 the rough sea made evacuation difficult and if a decision had not been taken to beach the LSTs, the evacuation of casualties would have ceased and the CEPs would have been overcrowded.
The policy of using medically adapted LSTs, and setting aside DUKWS for medical purposes worked extremely satisfactorily; there were, however, misunderstandings and difficulties concerning the arrival of hospital carriers. Eventually it became routine for an officer of the CEP to meet the carriers in a DUKW and guide them to the proper anchorage.
By 26 July 38,581 casualties (including sick) had been evacuated to UK by sea.
Evacuation by air began on 13 June which was a week. earlier than had been anticipated in planning.
Air evacuation was more uncertain than sea evacuation because the airfields on which suitable aircraft arrived changed constantly and there was always uncertainty as to the number of aircraft available. The problem was also complicated because no facilities existed on the air strip for holding casualties. Consequently no preparations could be made for evacuation until the aircraft had landed, and in a congested beachhead it was not always possible to deliver casualties at the air strip on time.
The necessity for dual documentation was another factor which caused a heavy strain on fighting units.
On 18 June ,however, the whole evacuation scheme was centralised under 11 L of C.
A Medical Air Liaison officer was attached to 83 Group RAF, 81 General Hospital, and later, 77 General Hospital at REVIERS was made the principal collecting centre for casualties to be evacuated by air, and a single air strip was selected for evacuation purposes.
RAF Casualty Air Evacuation Units began to arrive at this time and assisted in holding casualties on the airfield until aircraft were available. The holding capacity of these units was not large enough to deal with the numbers to be evacuated and on several occasions a FDS or CCS was sited to help out in this task. The number evacuated by air up to 26 July was 7,719.
MEDICAL STORES
There was no shortage of medical stores in the assault period and only minor losses of equipment occurred.
The system of supply over the beaches depended on the daily delivery of Medical Beach Maintenance Blocks, each composed of two half blocks weighing 25 cwts. and containing items of medical equipment designed to meet all reasonable demands until Advance Depots Medical Stores were established.
Two of these were sent over in split loads of five and ten tons between D+3 and D+10. This was considered necessary in view of possible sinkings. In addition six tons of medical equipment were preloaded on RASC transport to augment the medical maintenance blocks.
BLOOD TRANSFUSION
To meet the expected demands for transfusion fluids in the early days of the operation, the following arrangements were made :—
• Special issues of blood were made to the assault forces.
• Transfusion fluids were included in the maintenance blocks.
• FTUs landed with an estimated supply to last two days.
• Two Advance Blood Banks were landed on D+3 and allocated to each of the corps fronts.
• Supplies of whole blood were sent initially from UK by naval despatch launch and later from D+16 by air.
In a later stage of the campaign the two blood banks which had been allocated to the assault corps were put at the disposal of First Canadian and Second British Armies. These were supplied with blood from No. 1 Blood Transfusion Unit which landed on D+16 and set up at BAYEUX.
The supply to corps and divisional medical units was maintained by a daily service of trucks carrying blood from the army advanced blood bank. Penicillin was also distributed through the agency of the Blood Transfusion Service.
During this phase the following quantities of blood, plasma and penicillin were used : -
Blood . . . 18,000 pints
Plasma . . . 15,000 pints
Penicillin . . 2,400 mega units
EXHAUSTION
The incidence of cases of exhaustion rose steeply from the beginning of July (2.5 per 1000 per week) to the week ending 22 July (5.63 per 1000).
Enemy mortar fire was stated to be the main cause of the collapse of these psychiatric cases.
To deal with them Divisional Exhaustion Centres were opened, where casualties who could be quickly cured were admitted for four or five days. Corps Exhaustion Centres admitted casualties evacuated from divisional level for seven days’ treatment.
Beyond these at the Army Centres and at the Second Army Rest Camp men were treated and then given a period of convalescence.
Over 65 per cent of exhaustion casualties were returned to duty in the theatre. Of these 50 per cent returned to full duty, and the other 15 per cent to duty in a reduced medical category.
DENTAL
The employment of Mobile Dental Units at a distance of two or three miles in the rear of troops engaged in battle was fully justified, for the dentists were able to give treatment in the battle zone and retain the services of men of operational units, who would otherwise have been evacuated to the rear areas.
HYGIENE
The solution of hygiene questions did not present any serious difficulties. The water supply was not tampered with by the enemy, but required strict supervision. flies began to appear in large numbers and anti—fly precautions were improvised until fly-proofing materials arrived.
FEMALE NURSING
Nursing sisters began to arrive in the theatre from D+10 onwards. Their arrival was much appreciated because they improved the standard of post-operation treatment tremendously.
26 July-26 September
BUILD—UP OF MEDICAL BASE
In the early part of this phase the build-up of general hospitals continued in the medical area centred on RANCHY near BAYEUX. The personnel of hospitals arrived according to programme but the build-up was nevertheless disappointingly slow due to delays in the arrival of equipment.
This was shipped separately and owing to bad packing often proved deficient of small but essential items.
With one exception all hospitals at this stage were tented. The supply of Water was a major problem and even after a Water pipe line had been constructed Water carts were engaged full-time in delivering water within the hospital area.
Major medical installations in the bridgehead on 26 July amounted to twelve CCSs and nineteen general hospitals. In addition three Base Depot Medical Stores had arrived for the supply of medical equipment. By 26 September another seventeen general hospitals and two additional base depot medical stores had arrived.
One of the results of the slow build-up was that the policy of retaining patients in the theatre could not be carried out as early as it was Originally intended, and consequently during this period all patients who were fit to travel and who were unlikely to return to duty in one week were evacuated to UK.
MEDICAL LAYOUT PRIOR TO THE BREAK-OUT
Before the break-out First Canadian Army had two BRITISH general hospitals of 200 bed size at LA DELIVRANDE, which, aided by a 600 bed hospital at REVIERS, handled all casualties of l Corps.
2 Canadian Corps casualties went straight from the CCS area at ST GERMAINE to the main hospital area at BAYEUX. About 20 August the two 200 bed type general hospitals moved to the ST GERMAINE area which then became the nodal point for rearward evacuation from First Canadian Army. Second Army casualties coming back from FALAISE by-passed ST GERMAINE and Went straight back to BAYEUX.
In the main medical area Second Army hospitals remained closed in readiness to move forward.
MEDICAL LAYOUT AND CHANNELS OF EVACUATION OF CASUALTIES DURING THE PURSUIT
- FROM THE LINE OF THE SEINE
When the break-out occurred the evacuation line lengthened and a period of rapid movement and development of an air shuttle service began.
The battle of CAEN in August threw a great strain on the available number of hospital beds, but after the collapse of the enemy at FALAISE the picture changed completely. The heavy spate of casualties was for the time being finished but nearly 5,000 civilians were transferred from CAEN to other civilian hospitals, which movement fully occupied the ambulance car companies.
During the pursuit although only small rearguard actions were fought a great strain was put on the chain of evacuation: the great difficulty at this stage was lack of transport to bring hospitals forward sufficiently early.
This lack of transport was common throughout the Services and was inevitable in view of the nature of the operations.
As far as FALAISE and just beyond, all corps casualties were cleared by ambulance car company to BAYEUX. As the distance increased it was necessary to introduce staging posts and to obtain extra assistance from 227 MAC (8 Corps).
By the time the SEINE was reached the distance was far too great for large-scale evacuation by road, though a few cases were staged back via RUGLES and FALAISE. Most of the cases, however, were held by the general hospital which had opened at CAILLOUET until they could be evacuated by air from EVREUX.
On 5 September an ambulance railhead opened at MEZIDON, but four days later moved forward to LISIEUX.
Daily ambulance trains were organised from there to BAYEUX.
- FROM NORTHERN FRANCE AND BELGIUM
During the pursuit to the DUTCH frontier hospitals moved rapidly along the axes of both of the armies and by continually leap-frogging each other, ensured that the major medical services were always within reach of the forward troops and obviated the need for evacuating over long distances.
After the advance had gone beyond the SEINE and until BRUSSELS was reached, the chief method of evacuation was by Sparrow aircraft to the BAYEUX area, (the Sparrow flight consisted of six obsolete bomber Harrow aircraft).
The first air evacuation centre was at EVREUX, but this was soon moved forward to AMIENS where patients awaiting evacuation were held in the general hospital.
A few casualties were also evacuated from AMIENS by road to ROUEN, where a base hospital was established and a small number were sent by air from AMIENS direct to UK.
When BRUSSELS was reached there was at first only one way of evacuating and that was by air. Most of the cases went by Dakota aircraft to UK or were ferried by Sparrow to AMIENS. At a later stage casualties were despatched from BRUSSELS by rail.
When the DIEST area was opened the air shuttle evacuation service operated from DIEST to BRUSSELS and at the end of September was extended to EINDHOVEN.
The main method of coordinating casualty air evacuation was by direct liaison between DDsMS armies and the senior medical officers with the RAF groups. So rapid was the advance and so far were the corps removed from HQ Second Army that the DDMS had great difficulty in keeping the RAF fully informed of his requirements.
During the latter weeks of this phase steps were taken to set up a medical area at DIEPPE and later at OSTEND.
Evacuation WEST of the SEINE was planned to cease on 16 September when a daily hospital carrier service to UK from DIEPPE was instituted, but in fact it continued for approximately another week to enable the hospitals in BRUSSELS and AMIENS areas to be cleared in time to receive the expected heavy casualties of the ARNHEM airborne operation.
-EVACUATION FOR OPERATION MARKET GARDEN
The medical scheme for this operation reverted to the policy adopted in the beachhead of evacuating casualties from the theatre as quickly as possible. By 17 September two hospitals, both of 200-bed capacity, were established at DIEST, While another stood prepared in BRUSSELS, available either to open in an emergency on to move forward. A FDS was established in the DIEST area to assist the two hospitals.
The staging of casualties back to the medical area was under corps arrangements, while to assist in handling US airborne sick and wounded, an AMERICAN evacuation hospital and ambulance company was sited at BOURG LEOPOLD.
The holding capacity of the Second Army medical units when operation MARKET GARDEN started was far below that required to accommodate the estimated influx of casualties.
To overcome this problem of limited hospital accommodation 500-700 casualties were evacuated-daily by air from BRUSSELS to UK, and in addition a rail lift to AMIENS for 200~300 daily was organised.
An ambulance train formed from recaptured BRITISH and BELGIUM stock and staffed by BELGIAN Red Cross personnel made its first run from BRUSSELS to AMIENS on 20 September. To help in the evacuation of forward areas an additional ambulance car company was put at the disposal of the DDMS Second Army for the operation.
CASUALTIES EVACUATED TO UK
During this period a total of 26,039 casualties was evacuated to UK by sea and 20,964 by air.
WOUNDED PW
Many concentrations of wounded PW were over-run in BELGIUM. PW hospitals were opened at AMIENS, BRUSSELS, ANTWERP, and later at BOURG LEOPOLD, staffed by collecting all available GERMAN protected personnel.
STORES AND EQUIPMENT
When the move forward began the advanced depots medical stores were re-sited in accordance with the new positions of the corps which each served, but the system of supply based on geographical layout had to be altered to meet rapidly changing conditions.
The advanced depots medical stores could not move at the speed required to maintain a satisfactory supply system.
To overcome this, mobile elements were formed from the depots, consisting each of two three-ton lorries and a supply of medical equipment.
The mobile element was attached to the forward CCS of the corps normally served, and proved a satisfactory answer to the problem.
Following the battle of the FALAISE gap the moves of the advanced depots medical stores were long and frequent. One was retained at AUBIGNY to supply units in the rear, while the others were “leap-frogged” forward into BELGIUM. Two of those depots moved up to NIJMEGEN and EINDHOVEN in support of the MARKET GARDEN operation.
Depots were based for maintenance on base depots medical stores at BAYEUX and at DIEPPE.
GENERAL HEALTH OF TROOPS
Towards the end of July and in the early days of August there was a marked increase in enteritis and diseases of the digestive system. This was undoubtedly caused by the large increase in the fly population, due to the very crowded conditions in the bridgehead, and to the existence of hundreds of unburied carcasses of cattle.
In September as troops moved forward into unsoiled ground there was a distinct drop in the incidence of enteritis. A certain amount of malaria made its appearance, some of which was probably caused by troops transferred from the ITALIAN theatre.
The rate of VD rose from .43 per 1,000 per month in August to .74 per 1,000 per month in September.
An outbreak of typhoid fever which was immediately localised occurred in HQ 6 Guards Tank Brigade.
Seventy-three cases were reported up to 26 September, all from Brigade HQ.
This was the only real epidemic of the campaign so far and was believed to be due to a carrier in contact with the HQ personnel.
27 September 1944—14 January 1945
BUILD-UP OF HOSPITALS NORTH OF THE SEINE
The quick advance of the armies had left the majority of the hospitals in the RMA. It was therefore of primary importance to move at once as many as possible into northern FRANCE and BELGIUM, since at the beginning of this period there were only 6,100 beds to serve the bulk of 21 Army Group located NORTH of the SEINE, compared with the 11,400 beds which remained in NORMANDY.
Despite the urgency of the situation only one general transport company could be allotted to the task and this was fully employed up to the end of December in moving the required medical units forward.
Apart from the lack of transport, the speed at which the hospital area in the advance base was built up also depended on finding and adapting adequate covered accommodation, for since winter was approaching, it was not feasible to site hospitals under canvas.
At one time the lack of accommodation was so serious that six general hospitals which had become redundant in the RMA were shipped back to UK to wait until suitable buildings were available in the advance base.
The problem was gradually surmounted by taking over all existing civilian and GERMAN military hospitals and by converting many large schools and convents to medical uses. By 7 January 29,600 beds were equipped and functioning within the theatre, while 1,400 beds were closed but ready to open when required.
HOLDING POLICY AND CONVALESCENT DEPOT
At this time the lack of adequate convalescent depot facilities adversely influenced the intention to lengthen the holding period.
Nevertheless by 27 October cases which were likely to return to duty or to be convalescent within twenty-eight days were, whenever possible, held in the theatre, and by 7 December the holding period had been extended in most cases to thirty days.
The opening of convalescent depots was delayed by lack of suitable accommodation, the need to wait until completion of the necessary engineer work, and the difficulty in obtaining essential accommodation stores such as beds or double bunks.
A 500 bed depot was eventually opened at ST POL on 30 October and another with a capacity of 300 beds at DE HAAN in November. By the first week in January 3,700 beds were available in convalescent depots.
L OF C
Hospital Areas
The main hospital areas in the L of C were in the vicinity of BRUSSELS, ANTWERP, GHENT, BRUGES, OSTEND, LILLE, TOURNAI, AMIENS and ST OMER.
Early in the period there were hospitals at ROUEN and DIEPPE.
When US forces took over these areas and when DIEPPE closed as a port these medical units moved into BELGIUM.
The medical area of the RMA which figured so importantly in previous phases now existed only in the shape of a winterised 1,800 bed general hospital in BAYEUX.
Evacuation
Evacuation by hospital carrier from the RMA continued from ARROMANCHES until mid December, although by this time the commitment had dwindled to only one carrier weekly.
When this service ceased casualties unfit for evacuation by air were accepted by the US authorities and taken to UK from CHERBOURG.
Air evacuation continued from CARPIQUET, but by the end of the year it was more usual for casualties to be shuttled forward to an airfield near ST OMER.
Hospital carriers continued to evacuate casualties NORTH of the SEINE from DIEPPE until mid November, but the main port for sea evacuation was OSTEND which despatched its first hospital carrier on 21 October.
Movement to OSTEND from other hospital areas was through ambulance railheads.
The BRUSSELS area which received shuttle cases from Second Army and also, until early November, most of the ambulance trains, was the main centre for air evacuation.
Air evacuation from ANTWERP started at the beginning of October, but as ANTWERP became untenable as a medical centre, due to attacks by V Weapons, the air evacuation unit was moved to BRUGES and continued to function from there.
SECOND ARMY
Medical Areas
Early in October two general hospitals (200 beds) and one 600 bed general hospital set up a medical area in the vicinity of EINDHOVEN, which continued to receive the casualties from various winter operations. A CCS was sited near the airfield at EINDHOVEN to act as a holding unit for the “air cushion”.
The US Evacuation Hospital was moved NORTH of UDEM to deal with US casualties from NIJMEGEN and eventually returned to US control in December.
In mid November in order to provide hospital facilities for the operations in which 12 and 30 Corps were then employed NORTH of SITTARD, a subsidiary medical area consisting of one 200 bed and one 600 bed hospital was set up at HASSELT.
This area later received the casualties from the BRITISH divisions employed in the ARDENNES battle. A convalescent depot (1,000 beds) opened at BOURG LEOPOLD in mid November and its presence enabled Second Army to carry out a fourteen days holding policy within its own medical area.
Evacuation Channels
Early in October the air shuttle service moved to EINDHOVEN and remained there throughout the period.
Cases which required a long term of treatment and convalescence were evacuated direct to UK, and other cases to BRUSSELS.
From the BRUSSELS area personnel trains transported sitting cases to the AMIENS area two or three times a week.
The first army ambulance railhead was established at OVERPELT when casualties were loaded on temporary ambulance trains, consisting of box cars fitted with stretchers.
The ambulance railhead moved forward to VALKENSWARD on 10 October and at the same time properly fitted ambulance trains which had come forward across the SEINE were put into use.
Although the emergency ambulance trains had greatly assisted in clearing casualties they did not form a satisfactory method of handling patients who where seriously ill. Rail evacuation continued to BRUSSELS until November, after which it was possible to run trains direct to all the L of C medical areas.
During the ARDENNES counter offensive casualties of 30 Corps were evacuated direct into hospitals at BRUSSELS and LOUVAIN. The hospitals in this area were cleared of all casualties and their holding policy shelved during the time of the crisis.
First Canadian ARMY
At the beginning of this period two general hospitals (200 beds) under control First Canadian Army were situated at COURTRAI and ANTWERP.
Casualties from CALAIS were evacuated direct to a general hospital (600 beds) at ST OMER, and those which occurred in the fighting in the LEOPOLD canal area were sent to ANTWERP and BRUGES.
Casualties from the WALCHEREN operation were evacuated from field ambulances direct to hospitals in GHENT and BRUGES, although some were evacuated by sea direct to OSTEND.
By the end of December the main concentration of hospitals in the First Canadian Army was situated in the ’s HERTOGENBOSCH-TILBURG area.
Ambulance trains began to run from TURNHOUT on 7 December, while air evacuation direct to UK by Dakota and to BRUGES for short term cases by “Sparrow” flight began on 12 December.
US CASUALTIES
The casualties of 82 and 101 US Airborne Divisions were handled by 24 US Evacuation Hospital, who used BRITISH channels of evacuation.
Early in January when the ARDENNES operation put a strain on US medical arrangements, an offer was made to clear the US hospitals in NAMUR and LIEGE by BRITISH ambulance trains to OSTEND, but although the offer was accepted it never became necessary for the plan to be put into effect.
SUPPLY OF MEDICAL STORES
Base depots medical stores continued to be centred in the areas TOURNAI, ANTWERP, OSTEND, BRUSSELS and LOUVAIN, while advanced depots medical stores supplied the needs of their respective armies.
The Base Blood Transfusion Unit was situated at BRUSSELS where it received daily supplies of blood by air.
HEALTH OF THE TROOPS
The health of the troops remained at a satisfactory high level; in spite of the changing conditions of accommodation and ground, standards of sanitation were well maintained.
From the time the troops ceased to live in bivouacs and were accommodated in billets or other buildings, there was some increase in colds and mild respiratory diseases.
There was a sharp rise in VD rates which coincided with the entry into the populated areas of BELGIUM and HOLLAND and the commencement of leave on the Continent.
The incidence rose throughout the period and while the mean monthly rate per 1,000 troops was 1.98 in October, it had risen to 3.06 in December.
There was also a rise in the scabies and pediculosis rate.
The monthly rate of sick admitted into hospital was :—
- October — 22.4 per 1,000 men
- November — 24.3 per 1,000 men
- December — 28.0 per 1,000 men
In November the first twelve cases of trench foot to appear in the theatre were reported, and by December another fourteen new cases had come to light. This incidence can be counted as negligible, especially as each case was only a slight attack.
The almost complete absence of this type of casualty can be largely ascribed to good man-management by regimental officers coupled with the issue of socks on a generous scale to forward troops.
Statistics showing admissions to medical units and the incidence of certain diseases are found at Appendix “N” not yet ready.
15 January 1945 - 8 May 1945
BUILD-UP AND HOLDING POLICY
Hospital bed accommodation was increased to the extent of one 1200 bed general hospital which arrived from UK in January and one BRITISH and two CANADIAN (600 bed) general hospitals which arrived in March as part of operation GOLDFLAKE.
At the end of the campaign there were 36,100 hospital beds in the theatre. The highest number which functioned in any one day in the L of C was 32,385 on 23 April.
The remaining beds were either forward with armies or closed waiting to move. On VE day beds in convalescent depots in the theatre totalled 12,200.
The general manpower shortage was substantially overcome as far as the supply of medical personnel was concerned by employing VAD and ATS personnel who were posted to general hospitals in steadily increasing numbers from March onwards.
By 8 May the total number so employed was approximately 1,200 of which 450 were VAD members.
On 11 February the period for holding casualties and patients on the Continent was extended to forty-two days. It was never possible to institute the sixty day holding policy which had been envisaged in the original planning of OVERLORD.
L or C
HOSPITAL AREAS
Although a considerable number of units moved forward into GERMANY during the latter months of the campaign, BELGIUM continued to be the main medical base up to the close of operations. As the number of troops in the RMA diminished, the hospital accommodation was correspondingly reduced and the general hospital at BAYEUX was moved into BELGIUM by the end of March, leaving a FDS reinforced by certain specialists to supervise a 300 bed hospital.
A small camp reception station had been established in PARIS for BRITISH troops stationed there on leave. All those who required hospital treatment were sent to US hospitals.
AMIENS was cleared of hospitals in April leaving LILLE and ST OMER as the only hospital centres still in use in FRANCE. Casualties from the force containing DUNKIRK were evacuated direct to the CANADIAN hospital at ST OMER.
TURNHOUT was developed as a CANADIAN base hospital centre, initially with one 600 and one 1200 bed hospital, but in March the 600 bed hospital was replaced by another 1200 bed unit.
A convalescent depot for women’s services was set up in BRUSSELS early in March and the convalescent depot at ST POL moved to HASSELT early in April.
Medical arrangements for operation GOLDFLAKE consisted of medical officers and ambulance cars from the formations arriving from ITALY, being sited at various staging camps along the route to the BRITISH sector.
One FDS was established at MARSEILLES and another FDS formed two camp reception stations at the northern end of the route. MI room facilities were provided at the other camps, and cases requiring hospital treatment were admitted to US army hospitals. One field sanitary section and sets of medical equipment were provided from 21 Army Group sources.
EVACUATION
Evacuation from the L of C hospital areas to UK continued by sea from OSTEND and by air from BRUSSELS, MALDEGEM, and occasionally LILLE. Railway facilities within the theatre were such, that up to the time of the RHINE crossing casualties of the two armies could be despatched almost direct from the fighting fronts to the various L of C hospital centres.
There were eleven BRITISH ambulance trains and one BELGIAN Red Cross train connecting the main medical areas in the advance base. Within the L of C two diesel-engined ambulance rail cars, each with a capacity of about thirty patients, started to operate on 24 March and proved invaluable in collecting and distributing patients between the centres of air evacuation and outlying hospitals.
They also made journeys from BRUSSELS to deliver US patients to hospitals at LIEGE and to collect BRITISH personnel who had been evacuated through US medical channels.
The majority of road evacuation immediately behind the armies was undertaken by two RASC ambulance car companies, assisted by a third manned by AMERICAN Field Service personnel which arrived from CMF in April.
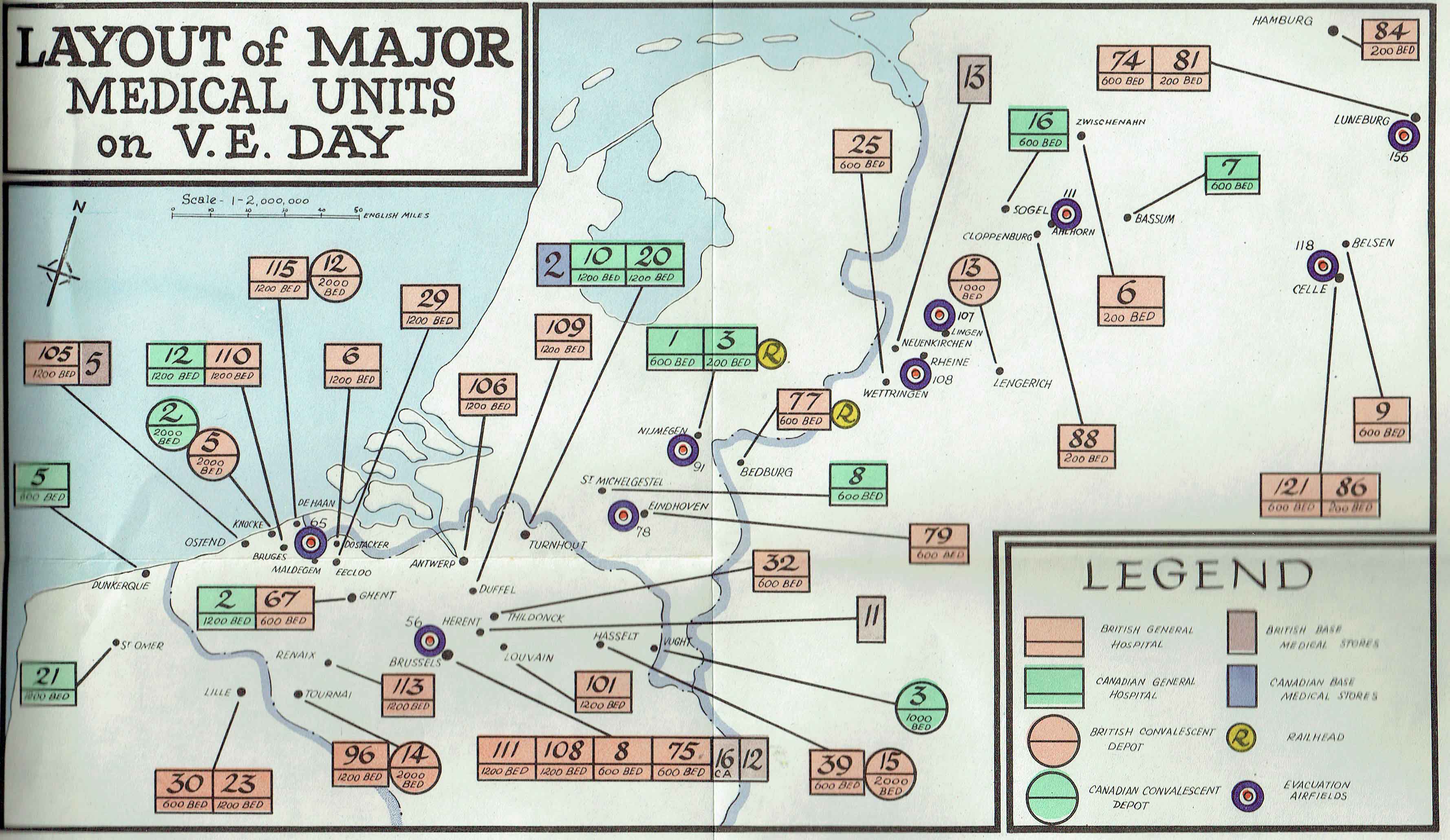
A map illustrating the final layout of major medical units and centres of evacuation is shown here
During the campaign 77,317 (including 89 PW) patients were evacuated to UK byair and 89,397 (including 18,911 PW) cases by sea. Within the theatre 39,335 cases were moved by air 83,799 (including 11,676 PW’) by rail, and 450,7 71 by road.
SECOND ARMY
MEDICAL AREAS
There was no need to make major alterations in the main hospital areas at EINDHOVEN and HASSELT for operation VERITABLE. Medical facilities of 2 Cdn Corps and 30 Brit Corps were pooled for the operation, while a number of Second Army medical units, including three CCSs, eight FSUs and five FTUs were put at the disposal of First Canadian Army for 30 Corps.
An additional motor ambulance convoy was also lent for a period. As operation VERITABLE progressed the Second Army hospital areas at EINDHOVEN and HASSELT were reduced in size and a forward hospital area, consisting at the end of March of one 600 bed hospital and two of 200 bed capacity, was established at VENRAIJ. A blood bank and an advanced depot medical stores were also sited in the area.
Ambulance evacuation from corps medical installations WEST of the RHINE in the early stages of operation PLUNDER presented no problems as the hospital area at VENRAIJ was easily accessible from the main traffic routes crossing the River MAAS.
For the crossing of the RHINE each assault corps was allotted one light field ambulance, to organise and control evacuation within the bank control group area. Before bridges were constructed over the river, evacuation from the EAST bank was achieved by specially allocated DUKWS, Buffaloes, Weasels and other available craft.
Casualties were evacuated to CCSs set up in the area of BEDBURG and KAPELLEN. Provision was made for casualty evacuation of US troops during operation VARSITY by a platoon of a US field hospital also sited at KAPELLEN. As it was impossible to sortout casualties into nationalities on the far bank of the RHINE it was arranged that casualties would be evacuated through joint BRITISH US channels until the CCS area was reached.
After the RHINE crossing there was continuous movement of one hospital after another, reminiscent of the advance through FRANCE, in an attempt to keep major medical facilities close to the fighting troops.
200 bed general hospitals and CCSs were moved forward in army transport, while the larger hospitals were sent forward under HQ 21 Army Group arrangements. The allotment of a GT coy for medical purposes,supplemented by various additional lifts and aided by rail movement for part of the way, meant that a much speedier move forward was possible than in the break-out in NORMANDY. The accommodation problem caused no difficulty for the weather was fine enough for tentage to be used when buildings were not available.
CHANNELS OF EVACUATION
An ambulance railhead moved forward to HELMOND on 18 March and to SEVEN UM, which was conveniently close to VENRAIJ, on 24 March. In addition to the normal allotment of one ambulance car company for casualty evacuation within the army and corps area, HQ 21 Army Group made two further platoons of ambulance cars available to Second Army for operation PLUNDER.
For evacuation by rail it was planned to make one ambulance train available at the railhead on D-day and, there after, two ambulance trains daily as long as required.
Successful air evacuation from HEES, which reached an average of four hundred daily, made it possible, however, to cut down the number of trains to one per day after four days. The railhead finally moved to BEDBURG in April. No ambulance trains crossed the RHINE before hostilities ceased but arrangements were made to have running rights across the US railway bridge at WESEL if required in an emergency.
From early in April the number of casualties evacuated by rail rapidly decreased because the long road journey back to ambulance railhead from the forward areas was a strain for even the lightly wounded. Evacuation from forward areas was achieved by air shuttle service direct to BRUSSELS.
Several ambulance trains with FRENCH and BELGIAN sick, ex-PW and DPs were run from BEDBURG.
At the end of March the air shuttle service had moved from EINDHOVEN to HEES and on 10 April was moved forward to RHEINE.
On 18 April air evacuation facilities were available from CELLE and DIEPHOLZ and on 1 May from LUNEBURG.
Casualties on the left flank of Second Army were evacuated from the CANADIAN airfield at ALHORN.
FIRST CANADIAN ARMY
MEDICAL AREAS
One BRITISH 200 bed hospital at TILBURG, one 200 bed and one 600 bed CANADIAN hospital at ’s HERTOGENBOSCH, served as the main CANADIAN forward medical area during January and February. During operation PLUNDER a CCS was sited at BEDBURG to receive casualties from 2 Cdn Corps. After the crossing of the RHINE, CANADIAN medical units moved in support of First Canadian Army in a similar manner to Second Army hospitals.
EVACUATION
During operation VERITABLE the CLEVE-NIJMEGEN road, along which casualties were evacuated, was flooded.
From 13 February-18 February and to some extent until 28 February, casualties were therefore despatched to the CCS at CLEVE by DUKWS.
On 29 January a CANADIAN ambulance railhead had opened at ’s HERTOGENBOSCH. It was forced to close down on account of enemy action and re-opened at BOXTEL on 1 March. It moved again to NIJMEGEN on 4 April and remained there until the end of the campaign.
The main airfields used by the shuttle service in the advance into GERMANY were KLUIS, LINGEN and finally ALHORN
OCCUPATIONAL PROBLEMS
Ex PW AND DISPLACED PERSONS
It was the responsibility of the Medical Services to examine all BRITISH and US PW and to dust them with de-lousing powder before they were evacuated to UK.
In addition, by 8 Way 919 ex-PW had been evacuated through medical channels. The responsibility for Displaced Persons was primarily that of the Military Government authorities, but great assistance was given by the military Medical Services in providing hospital. facilities and in supervising the hygiene and sanitation of DP camps.
In order to prevent the spread of disease in EUROPE, all DPs and ex-PW entering BELGIUM or southern HOLLAND from the EAST were detained in camps at the border, where they were examined and dusted with de-lousing powder before they were allowed to proceed. This sanitary cordon which was later extended to the RHINE-IJSSEL rivers, was so effective that few cases of disease were reported which could be traced to contact with repatriated persons.
THE GERMAN ARMY
The GERMAN military hospitals which were over-run in the advance were full of wounded.
No casualties were, however, evacuated from GERMANY after the RHINE had been crossed. As the GERMAN administrative system was completely disrupted, groups of WEHRMACHT hospitals were supervised by BRITISH medical units for purposes of control and organising supply.
Between five and twelve GERMAN military hospitals were put under the supervision of a field ambulance or FDS. The problem of controlling large numbers of captured GERMAN hospitals increased as the advance continued. Eventually MUNSTER LAGER, WINSEN, DELMENHORST and LUNEBURG became the main centres for holding GERMAN wounded.
The total number of prisoners of war in GERMAN hospitals in the army area amounted to 134,000 at the time of the ELBE assault. Two captured enemy medical equipment sections which had been formed earlier in the campaign and which had been sorting captured medical equipment in BELGIUM were brought into GERMANY to locate and concentrate the GERMAN medical store depots.
CONCENTRATION CAMPS
BRITISH medical units were called in to provide hospital, nursing and hygiene facilities at the concentration camps at SANDBOSTEL, FALLINGBOSTEL, NEUENGAMME and BELSEN which had been discovered in Second Army area.
The largest and most notorious camp, at BELSEN, was taken over on 15 April when the death rate was allegedly as much as five hundred cases per day.
One CCS, one light field ambulance, two field hygiene sections and a mobile bacteriological laboratory were sent there, followed later by a 600 bed general hospital, BRITISH Red Cross Society relief teams and other voluntary relief teams.
By 8 May accommodation had been found for nine thousand hospital cases and the death rate had fallen to approximately 110 per day.
MEDICAL SUPPLY
For most of the period medical units continued to be supplied from the advance base but base depot medical stores moved from TOURNAI to NEUENKIRCHEN early in April to be nearer both armies. The blood supply to the armies continued to be made from the base transfusion unit in BRUSSELS through advance blood banks with each army.
THE BRITISH RED CROSS SOCIETY
From the beginning of the campaign considerable assistance in providing extra comforts for the welfare of patients, was given to the Medical Services by the joint War Office organisation of the British Red Cross Society and the Order of St John of Jerusalem.
Lady welfare officers were attached to all hospitals, convalescent depots and, latterly, to CCSs. They provided an abundant supply of books, toilet requisites, cigarettes and games, as well as small articles of furniture, clothing and equipment which were not usually obtainable from army sources.
Three BRCS ambulance car platoons assisted RASC ambulance car companies in carrying on casualty evacuation in the L of areas. The work of a BRCS chiropody unit working in the OSTEND and ANTWERP areas was so valuable that arrangements were made for two more to besent from UK.
The BRCS Commission established two hostels, one in BRUSSELS and one in OSTEND to accommodate the relatives of dangerously ill patients. By agreement with the War Office a scheme for bringing relatives of dangerously ill patients into the theatre commenced on 15 March.
Two BRCS convalescent homes one for male and one for female officers were opened in BRUSSELS and two further convalescent homes were set up on theBELGIAN coast in the second half of May.
HOSPITAL VISITS
During February a scheme for local English speaking ladies to visit hospitals was inaugurated in BELGIUM under the auspices of the wife of the British Ambassador and had a considerable effect in raising morale of patients.
The scheme was later extended into FRANCE and HOLLAND.
Abbreviations
To see more abbreviations https://www.ww2history.eu/abbreviations
